RESEARCH WEEKLY: The ‘national bill’ for severe mental illness
(Jan. 21, 2016) The study of mental health is characterized by what is known as the “evidence-to-practice” or “science-to-treatment” gap. “Chasm” would be more fitting.
Around the world, thousands of scientists and academics are at work to explore and define the causes, mechanisms and treatments of psychiatric diseases and to examine the public health, policy, economic and other impacts of them. Yet few of these discoveries make their way into general public awareness and usefulness.
The gap has huge practical implications. Hypotheses are being tested, treatments are being tried, and evidence is being amassed that directly bears on the everyday lives and work of patients, families, clinicians and policymakers, who don’t learn about it in a timely way – or at all. RESEARCH WEEKLY was launched by the Treatment Advocacy Center as one small step toward bridging the gap. When we publish and distribute a blog like “Fish oil may delay onset of schizophrenia,” it is our contribution to getting treatment evidence into the hands of people who could benefit from it. When we calculate the risk mental illness adds to police incidents in a study like “Overlooked in the Undercounted: The Role of Mental Illness in Fatal Law Enforcement Encounters,” it is because lawmakers cannot make evidence-based policy without evidence.
FIGURE 1: The National Bill for Schizophrenia Hospitalization, By Payer (2013)

The Cost Factor
One of the many factors that influence the transfer of evidence to policy or practice is money. From city halls to the halls of Congress, the savings or cost associated with treating or not treating people with severe mental illness is often decisive in whether treatment policies and practices fly or die. Fortuitously, when it comes to the single biggest driver of direct costs for severe mental illness – hospitalization – the federal government itself operates a robust and user-friendly resource.
The Healthcare Cost and Utilization Project (called HCUP) is “a family of health care databases and related software tools and products” operated by the Agency for Healthcare Research and Quality (AHRQ) within the Department of Health & Human Services. Among a multitude of data points, HCUP reports the cost of all hospital stays in the US – including mental health hospital stays – by year, region, state and many other variables. HCUP labels these aggregated costs “the national bill.”
According to HCUP, there were 1.2 million hospital stays for treatment of mood disorders and schizophrenia in 2013 (the most recent year reported,) and the “national bill” for this inpatient treatment was $28,344,368,387 – $28 billion, in rounder numbers. Mood disorders (primarily bipolar disorder and depression) accounted for the lion’s share of the absolute cost – $16.8 billion. With roughly half as many people diagnosed, schizophrenia was more costly per capita at $11.5 billion.
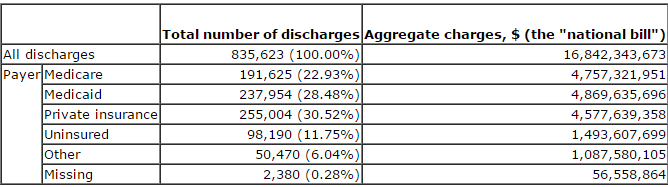
HCUP’s data shows that the public invests heavily in hospitalizing these critically ill patients. Through Medicare and Medicaid, the public paid 75% of the national bill for hospitalization related to schizophrenia and 50% of the bill for mood disorders in 2013 (Figures 1 and 2). The combined cost to Medicaid for hospitalizations related to the two conditions was topped only by the costs of hospitalizations for live births and septicemia (“blood poisoning”). At almost $9.2 billion, inpatient care for the two psychiatric diseases cost Medicaid more than twice what either respiratory failure or heart attack did.
FIGURE 2: The National Bill for Mood Disorder Hospitalization, By Payer (2013)
In the winter 2016 edition of Issues in Science and Technology, researcher Judith Teich writes, “Making progress on helping people with (serious mental illness) will depend not just on new drugs but on good information on which effective policies and treatment regiments can be based.”
Psychiatric hospitalization is the most expensive treatment modality that exists for severe mental illness. It takes place when psychiatric symptoms become so acute that inpatient care becomes a medical necessity, provided a bed is available. The national bill details the high cost that results when mood disorders and schizophrenia are not treated until psychiatric symptoms become so acute that inpatient care becomes necessary. It’s a resource that can help address the “service-to-practice” gap by providing “good information” for discussing “effective policies and treatment regiments” of two of the most disabling – and costly – psychiatric diseases.
References:
Treatment Advocacy Center. (11 August 2015). Fish oil may delay onset of schizophrenia.
Fuller, D. et al. (10 December 2015). Overlooked in the undercounted: The role of mental illness in fatal law enforcement encounters.
Healthcare Cost and Utilization Project. National statistics on mental health hospitalizations. Retrieved 12 January 2016.
Teich, J. (Winter 2016). Better data for better mental health services. Issues in Science and Technology.