Can a family member start an AOT program?

By Leslie Carpenter, Legislative Advocacy Manager, TAC
Can a family member advocate to start an AOT program? Absolutely! When we have a loved one with a severe mental illness (SMI) who doesn’t know they are sick due to anosognosia, it is a confusing and frustrating situation. We read books, connect with advocacy organizations, connect with advocates from across the country, and we learn what is happening elsewhere to help our loved ones. This is how I learned about assisted outpatient treatment (AOT) programs.
Eventually, I wrote an op-ed to address another issue related to how many people living with SMI are untreated in our country, and listed some of the solutions that could help.
The day that op-ed was published, Betsy Johnson, from TAC’s AOT Implementation Team, reached out to ask me if I would like to help improve Iowa’s commitment law to allow us to be able to do the work to start an AOT program. I obviously answered that we (my husband Scott and I) would love to do that.
This first step, which was to improve the commitment law in Iowa to allow AOT, proved to be a relatively fast process, thanks to Senator Joe Bolkcom and the many legislators in Iowa who helped us. We were able to accomplish this through an amendment to another, larger piece of mental health legislation moving forward in 2018. This was the easy part in our state; the harder part was getting a program started.
In Iowa, we had quite a few “problem-solving courts” of various types across the state that had been implemented via a variety of funding sources. Central court administration had a moratorium on creating any new specialty courts. This barrier felt huge, but I was determined to work around it. So I did, with the help of many others. I eventually became a volunteer lobbyist, advocated to increase the judicial budget, and developed a relationship with Iowa’s problem-solving court administrator and the key leaders in central court administration.
In the meantime, I received significant help from another state legislator, Representative Mary Mascher, to begin engaging with and securing buy-in from key stakeholders in our county. She suggested I provide a community talk at a public library in town, and she helped me to invite many of these stakeholders: community leaders such as city counselors, mayors, county supervisors, mental health providers, homeless shelter providers, substance use providers, law enforcement, the NAMI Iowa Executive Director (Peggy Huppert), people from the local NAMI Johnson County Board and Executive Director, people from the hospital, and more. (A full list of recommended stakeholders is listed in the white paper produced by TAC: White_Paper_FINAL_1.pdf)
After that, I began meeting with key stakeholders. At each meeting, I learned that there were more people for me to meet, and often each person would make email introductions to the next people. Eventually, the director of jail diversion for our county sheriff’s office agreed to be the leader of our planning committee and she took the lead in getting meetings planned. Sadly, she eventually left her position with the sheriff’s office, and our committee lost our leader. I sent an email out to others on the committee to ask one of them to step up. None did. We floundered and I started to wonder if we could find a way forward. Luckily, Betsy Johnson urged me to step up and assume that leadership role and assured me other family member advocates and NAMI members had been able to get AOT programs started, so she thought I could, too. She even had a NAMI leader in Ohio talk with me to give me a pep talk. It helped and I decided to do it. We resumed our regular meetings and kept moving forward.
Our first few attempts to get funding were unsuccessful. However, we eventually obtained funding to pay for a judicial referee in our county to work one day per week with our program as part of a formal funding request we eventually had approved and granted by the governing board and CEO of our Mental Health and Disability Services (MHDS) region.
After that, we rolled along working out logistics, hiring the program director, judicial referee and peer support specialist. The TAC team came to train our team in December 2022. The program director created the policies and procedures, and the team worked out logistics for the court paperwork and processes.
Our AOT program began in May 2023, and served 23 participants as of November of 2024. So far, for these 23 participants, hospitalizations were reduced by 73%, hospital days by 90%, emergency department visits by 77% and crisis stabilization days reduced by 53%. The total cost savings in costs avoided was $2,100,684. The program is just getting started, but people living with serious brain illnesses and anosognosia are starting to get the treatment they need, not to mention insurance, case managers and housing in some of the cases.
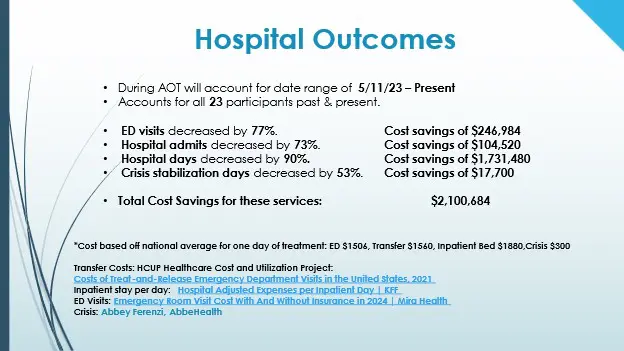
(This is a slide from a presentation provided at NAMI Iowa’s Annual Conference on November 21, 2024)
This all happened thanks to TAC’s wonderful AOT implementation team and their long-term help and support, and so many local people on our planning committee who stepped up to help implement the program. Teamwork…often by a few dedicated souls, is how we make progress. I am so grateful to every member of our team!


