Emergencies

Plan for a crisis by organizing paperwork and learning about state laws, local protocols, and disability rights.
Note: Treatment Advocacy Center is not a crisis intervention service and cannot provide emergency help.
What are the options in a mental health emergency?
911: If the situation is unsafe or medically urgent, call 911. Ask for a co-response team and request CIT-trained officers, if available. CIT refers to crisis intervention team training.
Mobile crisis: Mobile teams, typically staffed by mental health clinicians, are a good option when no violent behavior is present and there is a concern for self-harm.
988: The nationwide Suicide & Crisis Lifeline offers emotional support but may not be equipped to initiate a local, in-person mobile response.
Community Response: Community response programs dispatch specially trained, unarmed professionals to handle low-risk 911 calls related to poverty, mental health, substance use, or verbal disputes.
How might I prepare for an immigration-related encounter with federal agents?
Many rights organizations have concerns that people with disabilities, including those related to mental health, are vulnerable if approached, questioned, or detained by federal agents from U.S. Customs and Border Protection (CPB) or Immigration and Customs Enforcement (ICE). If a loved one with a disability is taken, contact a local immigration attorney or legal aid. Document interactions as comprehensively as you can.
The Native American Rights Fund (NARF) offers a downloadable flyer to read, print, share, and carry. Recommendations include what to do if you are approached in your car, at work, or in public and why you may want to carry a photograph of your birth certificate and/or passport in your phone, in case a state-issued or Tribal ID is not accepted as proof of U.S. citizenship.
Disability Solutions offers options to minimize harm:
-
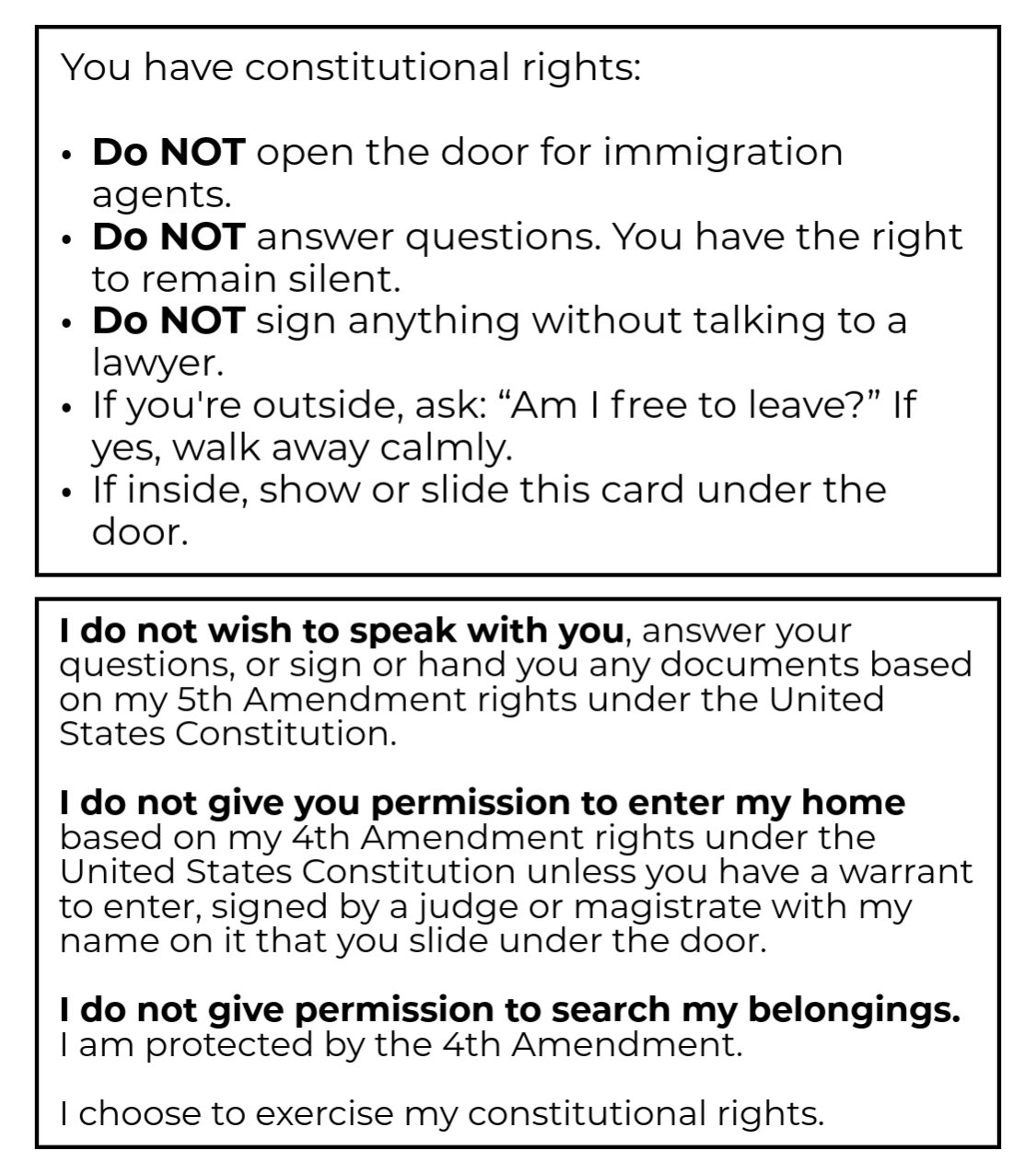
- Know your rights: Understand that you can remain silent and ask to speak to an attorney before answering questions or signing anything. Unless they present a warrant signed by a judge, agents are not authorized by longstanding law to enter your home.
- Plan what to do and say: Know how to use your personal electronic device to record an incident, and practice stating your rights out loud. A rights card can be printed and carried or stored in your phone.
- Plan to request disability accommodations: ICE is bound by Section 504 of the Rehabilitation Act, meaning that you have the right to request medical care, interpreters, and mobility support.
- Keep key documents in a “go bag” and be sure trusted helpers have copies:
-
- Photo ID
- Immigration paperwork
- Summary of conditions and treatment needs, i.e. mental health history
- List of medications and doctors
- Power of attorney or guardianship documents
- Rights card and attorney contact information
-
{kind=link}
Additionally, you can anticipate common questions by carrying a list of basic information, helpful if symptoms or cognitive deficits could make it difficult to respond verbally.
-
- What is your full name?
- Are you a U.S. citizen?
- Where were you born?
- How did you enter the United States?
- What documents prove your legal status in the United States? (List those documents and include statements about how you can show those documents or pictures of them.
How can I plan for a mental health emergency?
The goal is medical care, not criminalization. With that in mind, you will need to do some local research to determine the best number to call for a specific emergency.
Call a service agency: If the person in distress has an outpatient provider, an emergency hotline connected to that agency is a good first choice, if available. Find out if it is a 24/7 service or if there are limited hours. Note how long you might expect to wait for in-person response.
Call county crisis: A county hotline is a good next choice. Request a mobile crisis response team—and make a note if there is a specific name for a local team. The Right Response Directory may include a program near the person in crisis, or a county website might have information about local services. Some teams include a partnership between mental health clinicians and law enforcement for a “co-responder” approach. A team may utilize various professionals and peers, who provide emotional support informed by lived experiences.
Non-emergency police number: Calling local law enforcement at a non-emergency number can also be an option, whether the person in distress is someone you care for or a stranger. When you call you can ask if there is a mobile crisis or community response option. Explain that you are concerned about the person’s well-being. Be sure to provide a description of the person, symptoms you have witnessed, and their exact location. If law enforcement is the only responder option, request officers with CIT training. Say this: “Please send CIT-trained officers.”
Know what else is available: To research alternatives to law enforcement, look online:
- To find cities with community response programs, search on the website for Law Enforcement Action Partnership.
- To seek a mobile crisis program, check the Right Response Directory.
What do I do if the crisis response doesn’t help?
If a mobile crisis team responds but leaves without enabling stabilization or treatment for your loved one, plan to call again—and again—and again. You are creating a record of the crises, and not all responders will approach the situation the same way.
More about 988
988 is the nationwide Suicide & Crisis Lifeline, providing emotional support by phone or text. However, it may not be able to initiate an in-person response, and counselor training varies by location. As a result, counselors may not always be equipped to guide care partners when a loved one, in psychosis, cannot communicate their needs. Use a contact form to request information or express concerns related to 988.
If you call, text, or chat 988 to connect with a crisis counselor, services are immediately available in English and Spanish, with interpretation upon request for other languages. The 24/7 call center is confidential and free. Those who are deaf, hard of hearing, and TTY users can use preferred relay service or dial 711 then 1-800-273-8255.
Veterans can press 1 to be directed to a specialist in veterans mental healthcare. The 988 website includes resources specifically for veterans.
More about CIT
Crisis Intervention Team (CIT) training is best known for de-escalation, but its purpose is broader. CIT fosters collaboration among law enforcement, mental health and substance use professionals, and individuals and families with lived experience. According to CIT International, the model reduces stigma and unnecessary justice-system involvement while creating a framework for effective problem-solving and sustainable change.
Will 911 work if I live somewhere different from the person in crisis?
Maybe. You can call and request a transfer. A dispatcher will work faster if you have an exact location for the person in crisis—a street address with city, state, and zip code—along with their telephone number.
When planning for the possible emergency, check the website for the police department where the person in crisis lives. Look for a 10-digit emergency number, sometimes called the public safety answering point (PSAP). If you cannot find this number, call the non-emergency number for the police department, and say: “I need the 10-digit number to call in case of an emergency or for a transfer to dispatch.”
Save the 10-digit number with your emergency checklist (see below).
Can an emergency be used to initiate court-ordered mental health care?
If the person in crisis lacks awareness that they have SMI, common when they have a symptom called anosognosia, they may insist there is nothing wrong, despite symptoms and concerning behaviors that are obvious to others. In those situations, an emergency might lead to a frustrating stand-off between the person who is ill and those attempting to help. It also might be the first, best chance to shift a person toward mental health care that can lead them to recovery.
Planning an approach for care increases the chances for a helpful outcome, and the first thing to learn is state law. Look up your state on TAC’s interactive map to read the treatment laws that relate to emergency evaluation, inpatient and outpatient commitment. TAC provides additional information and a sample letter to adapt when seeking commitment for someone who is unable to access treatment independently.
Criteria for emergency evaluation are often, but not always, the same as the criteria for inpatient commitment and generally require a person to pose a danger to self or others as defined by the legislature. Danger to self always includes the risk of suicide or direct self-harm but can include other kinds of harm, such as grave disability.
Grave disability describes a person who is unable, due to mental illness, to provide for basic needs such as food, clothing, and shelter. In many states, grave disability includes being unable to appreciate the need for lifesaving medical care or to protect oneself from harm (such as walking into traffic). An increasing number of states include a risk for worsening psychiatric deterioration as part of the standard.
How might someone in a mental illness crisis be transported to a facility?
Every state has its own laws describing the criteria that must be met to transport someone to an inpatient mental health facility against their objection. How a person is physically transported depends on local service options and practices. Some areas rely on law enforcement, while others use ambulances or other secure medical vehicles. Sometimes, if it’s safe, a person can be transported by friends or family members.
Knowing ahead of time what is likely to happen and what is possible can create a more intentional approach. In North Carolina, for example, a clerk, magistrate, or district court judge can authorize a health care provider, family member, or friend to transport a person to a facility for involuntary treatment instead of law enforcement, which is the typical approach. The care partner may request to transport a patient by submitting a form to the clerk’s office.
Pro tip: Don’t count on system professionals to proactively share every available option. Take time to learn the policies, practices, and laws yourself so you’re prepared to ask for what your loved one needs before the crisis.
What might happen next, after transport for an emergency hold?
A person on an involuntary hold is taken to an inpatient facility. If there is no appropriate psychiatric bed available, they might stay in the emergency department or crisis facility. This is referred to as “emergency department boarding,” and has been an increasing problem as the number of psychiatric treatment beds continues to shrink.
Though theoretically an unstable person should not be discharged, many pressures incentivize hospitals to discharge patients as quickly as possible. Some hospitals deny care if a patient is “too acute” for their staffing model, even if there is an available bed. Other barriers may be related to insurance. TAC has additional information about discharge planning, including what to consider if there’s a risk for suicide.
Pro tip: Try to avoid premature discharge by promptly sharing mental health history, preferably by fax, with the facility. Share this information with each transfer; don’t expect these documents to travel with the person. If a premature discharge happens anyway, consider options for filing a complaint or for advocacy. Keep in mind that responding to constituent concerns is part of the job for elected officials and consider contacting a county or state official if that level of advocacy feels doable.
Is commitment a possible next step?
If the person is kept in the hospital and evaluated, the treating provider may determine that they meet criteria for continuing hospitalization—often called commitment. A provider’s petition to extend a hold triggers a judicial review. During that process, the patient has the right to be represented by an advocate or attorney.
Family members may be permitted to submit written or oral testimony for the civil court process in which a judge decides whether to order a commitment. The family can share information about the person’s condition, medical history, and/or recent behaviors. TAC provides additional information and a sample letter to adapt when seeking commitment.
Does commitment include medication?
In some locations, a judge may also rule on whether medication can be administered against objection. If medication against objection requires a court order that is separate from a commitment order, the family might advocate for hospitalization and treatment. An up-to-date medication log is an important tool for those circumstances.
How long will hospitalization last?
How long a person is held can be a fluid process. State commitment laws often allow a facility to hold a person for “up to” a certain time. Another civil court process is required to extend the stay. Hospital staff may quickly discharge a patient any time a new assessment determines that the person is no longer at risk for harming themselves or someone else.
Pro tip: Submit a letter of advocacy and mental health history at every decision point.
How do I build an emergency plan?
People often go blank during an emergency, so prepare an easy-to-find-and-follow checklist ahead of time (available for download at the bottom of this page). Having a plan in place can help ensure that the emergency is handled as a medical need for treatment—ideally avoiding criminal legal involvement. Periodically check the information in your emergency plan to ensure it stays up to date.
Checklist:
-
-
- Clearly labeled, with hours of operation, all numbers you might call in an emergency: 988, 911, local crisis hotline, local mobile crisis response service, long-distance 10-digit PSAP number (see above).
- Full address information for any location where a crisis might unfold.
- List of current or recent providers, with name, address, phone number: If a service agency has its own emergency response program, include that phone number and hours of operation.
- Psychiatric advance directive (PAD), if available: During times of stability, a person with SMI might write a PAD to share their wishes if they lose capacity.
- Quick facts about your state’s treatment laws and/or a drafted letter of advocacy with key words that draw a line between symptoms and behaviors and what is required for responders to issue an emergency hold and transport someone to a receiving facility.
- A list of who can petition for an emergency hold. This information is included in the state statute for emergency evaluation. In some states, a concerned community member can petition the court directly and in other states only certain professionals are authorized to petition. Print and store relevant documents about the petition process. If a credentialed professional is required, make sure that person is part of a crisis response team when you call.
- A list of who might transport a person to a receiving facility, such as law enforcement, mobile crisis, or a blended team. Print any relevant forms or petitions (required for family to transport in North Carolina, for example).
- Mental health history: TAC provides an article with a fillable form to help you keep a timeline of events, details about symptoms, and a medication record. Prepare to discuss how documented behaviors in the past have led to similar risks for harm. Share this form with first responders and with each and every facility providing evaluation and treatment.
- Photos and/or information about videos you have, with dates and location information, to use as evidence of symptoms, illness-related behaviors or threats, or a person at baseline to demonstrate a contrast. Share photos, videos, and other physical evidence in real time if possible, during an in-person response.
- Facilities in the area, with addresses, phone and fax numbers, that might receive someone put on an emergency hold: general hospital emergency department, psychiatric emergency room, crisis diversion facility, or somewhere else. Consider requesting transport to a facility of choice, if possible.
- Names, addresses, phone numbers for outpatient services that might be a good fit for discharge planning. Learning about options along the continuum of care can help with research to build this list. For example, is there an assisted outpatient treatment (AOT) program that might provide care under court order upon discharge? If yes, the time to start talking about AOT is upon admission.
-
A note on resources
In several places above we have detailed what is ideally available to address a crisis or emergency and next steps. As with almost all aspects of treatment and care for mental illness or substance use, what is available varies widely by location. There may or may not be a CIT trained unit where you live. You may find that even in locations where mobile crisis response exists there are not enough teams to serve the area in a timely fashion. 988 is a new system that is improving and growing quickly, but it will inevitably face bumps in the road in the same way 911 did when it was launched.
This reality provides an even greater incentive to do research on what is available where you live and plan. In an ideal world, all individuals and families affected by SMI would always have the full array of crisis services available. Until then, preparation and planning can help.